Abstract
Bullous pemphigoid /BP/ is a chronic blistering disorder that can affect oral mucosa very rarely. This autoimmune disease typically has a gradual onset and a chronic progressive course with exacerbations and remissions. Against components located in the epithelial basement membrane are formed autoantibodies. It is important to perform an incisional biopsy to establish a definitive diagnosis. Direct immunofluorescent findings are identical in BMMP and BP. Indirect immunofluorescence shows circulating IgG antibodies against the components of basement membrane in the majority of cases with BP but very rarely in patients with BMMP. There is no correlation between antibody titer and disease severity in BP. The aim is to present a very rare case of bullous pemphygoid of oral mucosa histologically proved with immunostaining. We present a patient with clinically identified oral lesion - bullae with clear fluid content in buccal mucosa of maxilla. After the rupture of bullae it left painful, superficial, ulcerated areas of oral mucosa. Hystopathological examination revealed subepithelial blister formation with clean separation of the full thickness of the epithelium from the underlying connective tissue layer. Direct immunofluorescence revealed a continuous linear band of immunoreactants at the basement membrane area. This immune deposit consist mainly IgG and C3, localized in the basement membrane. Conclusion: The treatment depends on the severity of the disease, tendency of progression and the affected areas. Therefore the clinicians should thoroughly examine all mucosal sites in order to make a proper diagnosis. The chronically characteristic of this autoimmune disease can lead to significant morbidity to patients. The adverse effects from long-term use of corticosteroids and immunosuppressives agents can also contribute to morbidity.
Keywords: Autoimmune, Pemphigoid, Ora,l mucosa, Oral, pathology, Histopathology, immunostaining
Received: 10 July 2018/ Revised: 14 August 2018 / Accepted: 19 September 2018 / Published: 1 November 2018
Contribution/ Originality
The paper contributes the first means-ends analysis of the connections of in-class simulation-based learning-performance by using the learning setting and participant-authored reports. Contrasted with previous studies which were essentially oriented in product/service decision-making, this study was built on the efforts to enhance the understanding of how the virtual management practices contribute to generation of personal values, rather than to focus on simulation system’s external validity.
1. INTRODUCTION
Autoimmune diseases typically have a gradual onset and a chronic progressive course with exacerbations and remissions. Mucous membrane pemphigoid (cicatrial pemphigoid) and bullous pemphigoid represents a group of chronic, blistering, mucocutaneous autoimmune diseases in which tissue-bound autoantibodies are directed against components of the basement membrane of the epithelium. This condition has a heterogeneous origin, with autoantibodies being produced against any one of a variety of basement membrane components, all of which are with similar clinical manifestations. It is interesting that these oral lesions seldom exhibit tendency for scar formation [1-4]. Bullous pemphigoid (BP) and cicatrial pemphigoid(CP) have similar causes and microscopic features but a different distribution of lesions. The skin in all patients with BP demonstrates large thick-walled bullae, but oral mucosal lesions are less common [5, 6].
Bullous pemphigoid is the most common of the auto - immune blistering conditions, occurring at an estimated rate of 10 cases per million population annually. In plasma of these patient could be found auto - antibodies directed against components of the epithelilium basement membrane. Bullous pemphigoid resembles in many aspects to mucous membrane pemphigoid, but most scientists note that there are enough differences between them to consider that these diseases as distinct but related entities. One of the significant differences is that the clinical course in most of the patients with bullous pemphigoid is usually limited, whereas the course in patients with cicatricial pemphigoid is usually protracted and progressive [7].
Direct immunofluorescent findings are identical in CP and BP. Indirect immunofluorescence reveals circulating IgG antibodies in plasma against the components of basement membrane in the majority of cases with BP but very rarely in patients with CP. There is no correlation between antibody titer and severity of disease in BP cases [5].
Oral mucosal lesions are almost always present, and they are the initial lesions in the majority of cases in patient with BP.
Bullous pemphigoid typically develops in patients between 60 and 80 years of age. No sex or racial predilection is generally reported. Pruritus could be an early symptom of the disease. This is followed by the development of single in the beginning and after that multiple bullae on either normal or erythematous skin. These lesions eventually rupture after several days and can cause a superficial crust. Healing takes place without scarring in most of cases.
Oral mucosal involvement is common, although the reported prevalence in several series of cases has ranged from 8% to 39%. The oral lesions, the same as the skin lesions, begin as bullae, but they have tend to rupture sooner, probably as a result of the constant low-grade trauma in oral cavity to which the oral mucosa is subjected. Large, shallow ulcerations with smooth, distinct margins are present after the bullae rupture [4, 7, 8].
Early lesions during the urticarial phase may be non-specific and show mild dermal oedema in the upper layers with perivascular infiltrate. Often conspicuous eosinophils could be found. Immunofluorescence is very helpful for diagnosis in this early phase of the disease. The blister that is formed is subepidermal and contains fibrin and also large numbers of inflammatory cells including eosinophils.
Aim The aim of our study is to present a rare case of BP with initial lesions in oral cavity.
2. CASE REPORT
During the scheduled visit to dental office a 54-year-old male was diagnosed with bullae in vestibular aspect of right maxilla. He was reported to the outpatient Department of Oral and Maxillofacial surgery, FDM, MU - Sofia, with a chief complaint of bullae. He has no history of difficulty in swallowing food or any eyesight problems. On general physical examination there were not any complaints and findings. On intraoral examination, a solitary intact bullae measuring about 5 mm in diameter was present on the upper labial mucosa.(Fig.1.) No other bullae and vesicles were founded. Based on patient's history and clinical presentation, a provisional diagnosis of mucous membrane pemphigoid was considered. After the rupture of bullae it left large, superficial, ulcerated, and denuded areas of mucosa.

Figure-1.The initial detected lesion
Source: Photo is taken by us- clinical case, that we describe
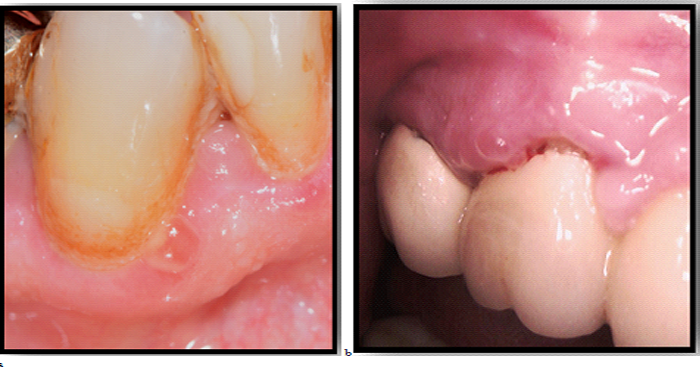
Figure-2. Bullous lesions of oral mucosa- a,b
Source: Photo is taken by us- clinical case, that we describe

Figure-3. Ruptured bullae
Source: Photo is taken by us- clinical case, that we describe
An incisional biopsy was performed from the affected area for histopathologic evaluation and for direct immunofluorescence test. Findings showed hyperplastic parakeratinized stratified squamous epithelium of irregular thickness with subepithelial split. Also biopsy of perilesional mucosa showed a split between the surface epithelium and the underlying connective tissue in the region under the basement membrane. Direct immunofluorescence showed linear deposition of IgG and C3 along the basement membrane.
After some days others lesions were presented in oral mucosa-Fig.2-a,b, fig.3
Direct immunofluorescence showed intercellular positivity for IgG and C3 and IgM, IG A, in the lining epithelium and acantholytic cells. Based on the history, clinical examination and the laboratory findings a definitive diagnosis of mucous membrane pemphigoid was confirmed.
Consultation with a dermatologist was performed for further treatment and follow up.
3. DISCUSSION
The etiology and pathogenesis of this disease is considered to be an autoimmune, with participation of epithelium basement membrane directed antibodies, that causes subepithelial separation.
Microscopic examination of tissue obtained from the perilesional margin of a bulla shows separation of the epithelium from the connective tissue at the basement membrane area, resulting in subepithelial blisters. Both acute and chronic inflammatory cells are typically seen in the lesional area, and also the presence of eosinophils within the bulla itself is most common feature [7].
Direct immunofluorescence studies reveal a continuous linear band of immunoreactants: IgG and C3, that are located in the basement membrane area in 90% to 100% of affected patients. These antibodies may bind to proteins associated with hemidesmosomes, structures that bind the basal cell layer of the epithelium to the basement membrane and the underlying connective tissue. It is interesting that these proteins in hemidesmosomes have been known as bullous pemphigoid antigens (BP180 and BP230). Immunoelectron microscopy has revealed the localization of BP180 to the upper portion of the lamina lucida of the basement membrane of the epithelium [7].
According some authors 50% to 90% of the patients also have circulating autoantibodies in the serum, producing an indirect immune fluorescent pattern that is identical to that of the direct immunofluorescence examination. The antibody titers seen in bullous pemphigoid do not appear to correlate with disease severity. The antibodies do not appear to be capable alone of inducing the lesions in this disease. Instead, binding of the antibodies to the basement membrane initiates the complement cascade, which in turn results in degranulation of mast cells, with recruitment of inflammatory cells like neutrophils and eosinophils to the affected area. The damage to the basement membrane is due to released by the inflammatory cells elastases and matrix metalloproteinases [6, 7, 9].
It is very difficult to distinguish mucous membrane pemphigoid from bullous pemphigoid, linear IgA bullous dermatosis or epidermolysis bullosa aquista. The distinctions could be made mainly on the basis of clinical findings. In the serum of patients with mucous membrane pemphigoid have been identified several possible target antigens. These include: bullous pemphigoid antigens 1 and 2; laminins 5 and 6; type VII collagen and ß4 integrin subunit [4, 10-12]. BMMP can also involve conjunctiva; nasal, esophageal, pharyngeal and vaginal mucosa; and skin as well. Adhesion and scarring between the bulbar and palpebral conjunctivae (symblepharon) can cause visual impairment (5). Bullous pemphigoid (BP) and BMMP have similar causes and microscopic features but a different distribution of lesions. The skin in all patients with BP demonstrates large thick-walled bullae, but oral mucosal lesions are less common. Direct immunofluorescent findings are identical in CP and BP. Indirect immunofluorescence shows circulating IgG antibodies in plasma against the basement membrane in the majority of cases with BP but only rarely in patients with CP. There appears to be no correlation between antibody titer and disease severity in BP [5]. Benign mucous membrane pemphigoid and bullous pemphigoid are clinically, histologically, and immunologically similar but differ in sites of involvement. Benign mucous membrane pemphigoid involves mainly the mucous membranes, most commonly affects oral cavity and next the conjunctiva. Skin lesions are infrequently observed. In bullous pemphigoid, the usual site of involvement is the skin. In approximately 30% of cases the oral mucosa is involved. The immunofluorescence pathologic findings in both diseases are identical, showing immune deposits along the basement membrane. However, the two diseases differ in the incidence and titer of basement membrane zone antibodies in sera. In bullous pemphigoid, basement membrane zone antibodies, generally of high titer (greater than I:80), occur in approximately 97% of patients. In benign mucous membrane pemphigoid, antibody titers (usually less than I:40) occur in only approximately 20% to 25% of patients [13-18].
The BP related complications can be decreased by its early detection and subsequent treatment. If only one mucosal site is affected, then a thorough review of symptoms highlighting involvement of other regions should be considered. The treatment of choice for patients with BP mainly depends on the affected site, progression and severity of the disease. A multidisciplinary approach has been put forth by the consensus group for its treatment. The multidisciplinary approach should include the dentists and dermatologist [19-22].
Other conditions can mimic pemphigoid histopathologically and differential diagnosis include: linear IgA bullous dermatosis, epidermolysis bullosa acquisita and angina bullosa hemorrhagica [3, 7].
In cases when epidermolysis bullosa aquisita is suspected the split skin indirect immunofluorescence examination could be very useful.
Treatment of the patient with bullous pemphigoid consists of systemic immunosuppressive medication. Management of the disease include moderate daily doses of systemic prednisone that usually control well the condition, following with alternate-day therapy to reduce the risk of corticosteroid complications. If the lesions do not respond to prednisone alone, then another immunosuppressive agent, such as azathioprine, may be added to the regimen. Tetracycline and niacinamide therapy is reported to be effective for some of the patients with BP. A sulfa derivative, Dapsone, may be used as an alternative therapeutic agent. The more severe, resistant cases require prednisone combined with cyclophosphamide; however, this regime has the potential for significant side effects [7].
The prognosis is generally good, with many patients experiencing spontaneous remission after 2 to 5 years. Problems may develop with immunosuppressive therapy in this older adult population, however, and mortality rates of up to 27% have been reported in some series [7].
4. CONCLUSION
The chronicity of the diseases can bring significant morbidity to patients. Adverse effects from systemic long-term use of corticosteroids and immunosuppressives also can contribute to morbidity for patients with BP. Because of heterogeneous pathogenetic mechanisms there is no single good therapy for every patient; treatment must be individualized, depending on lesional distribution, disease severity and progression, and therapeutic response to the disease.
| Funding: This study received no specific financial support. |
| Competing Interests: The authors declare that they have no competing interests. |
| Contributors/Acknowledgement: All authors contributed equally to the conception and design of the study. |
REFERENCES
[1] D. Williams, "Vesiculo-bullous mucocutaneous disease: Benign mucous membrane and bullous pemphigoid," Journal of Oral Pathology & Medicine, vol. 19, pp. 16-23, 1990.Available at: https://doi.org/10.1111/j.1600-0714.1990.tb00776.x.
[2] L. S. Chan, "Mucous membrane pemphigoid," Clinics in Dermatology, vol. 19, pp. 703-711, 2001.
[3] L. S. Chan, A. R. Ahmed, G. J. Anhalt, W. Bernauer, K. D. Cooper, M. J. Elder, J.-D. Fine, C. S. Foster, R. Ghohestani, and T. Hashimoto, "The first international consensus on mucous membrane pemphigoid: definition, diagnostic criteria, pathogenic factors, medical treatment, and prognostic indicators," Archives of Dermatology, vol. 138, pp. 370-379, 2002.Available at: https://doi.org/10.1001/archderm.138.3.370.
[4] W. Eveson, A. Cardesa, and P. J. Slootweg, Pathology of the head and neck. Springer, 2006.
[5] Peterson’s, Principles of oral and maxillofacial surgery, 2nd ed.: BC Decker Inc, 2004.
[6] N. J. Korman, "Bullous pemphigoid: The latest in diagnosis, prognosis, and therapy," Archives of Dermatology, vol. 134, pp. 1137-1141, 1998.
[7] B. Neville, D. Damm, C. Allen, and A. Chi, Sialolithiasis (Salivary Calculi; Salivary Stones). Adenoid cystic carcinoma. Oral and maxillofacial pathology, 4th ed. St. Louis: Saunders Elsevier, 2016.
[8] M. E. Eschle-Meniconi, S. R. Ahmad, and C. S. Foster, "Mucous membrane pemphigoid: An update," Current Opinion in Ophthalmology, vol. 16, pp. 303-307, 2005.
[9] O. Braun-Falco, G. Plewig, H. Wolff, and W. H. C. Burgdorf, Dermatology, 2ed ed. Berlin Heidelberg: Springer-Verlag, 2000.
[10] J.-C. Roujeau, C. Lok, S. Bastuji-Garin, S. Mhalla, V. Enginger, and P. Bernard, "High risk of death in elderly patients with extensive bullous pemphigoid," Archives of Dermatology, vol. 134, pp. 465-469, 1998.Available at: https://doi.org/10.1001/archderm.134.4.465.
[11] P.-J. Lamey, T. Rees, W. Binnie, J. Wright, K. Rankin, and N. Simpson, "Oral presentation of pemphigus vulgaris and its response to systemic steroid therapy," Oral Surgery, Oral Medicine, Oral Pathology, vol. 74, pp. 54-57, 1992.Available at: https://doi.org/10.1016/0030-4220(92)90215-c.
[12] R. Marsden, Linear IgA disease of childhood. In: Wojnarowska F, Briggaman RA Eds. Management of blistering diseases. New York: Chapman & Hall, 1990.
[13] M. Wood and P. Goaz, Differential diagnosis of oral and maxillofacial lesions, 5th ed. St Louis: Mosby, 1997.
[14] S. R. Parker and J. MacKelfresh, "Autoimmune blistering diseases in the elderly," Clinics in Dermatology, vol. 29, pp. 69-79, 2011.Available at: https://doi.org/10.1016/j.clindermatol.2010.07.010.
[15] A. Patsatsi, A. KyRIAKOU, A. Giannakou, A. Pavlitou-Tsiontsi, A. Lambropoulos, and D. Sotiriadis, "Clinical significance of anti-desmoglein-1 and-3 circulating autoantibodies in pemphigus patients measured by area index and intensity score," Acta Dermato-Venereologica, vol. 94, pp. 203-206, 2014.Available at: https://doi.org/10.2340/00015555-1666.
[16] E. M. Munyangango, C. Le Roux-Villet, S. Doan, F. Pascal, I. Soued, and M. Alexandre, "Oral cyclophosphamide without corticosteroids to treat mucous membrane pemphigoid," British Journal of Dermatology, vol. 168, pp. 381–390, 2013.Available at: https://doi.org/10.1111/bjd.12041.
[17] O. Gaudin, V. Seta, M. Alexandre, G. Bohelay, F. Aucouturier, S. Mignot-Grootenboer, S. Ingen-Housz-Oro, C. Bernardeschi, P. Schneider, and B. Mellottee, "Gliptin accountability in mucous membrane pemphigoid induction in 24 out of 313 patients," Frontiers in Immunology, vol. 9, p. 1030, 2018.Available at: https://doi.org/10.3389/fimmu.2018.01030.
[18] K. Nakama, H. Koga, N. Ishii, C. Ohata, T. Hashimoto, and T. Nakama, "Clinical and immunological profiles of 14 patients with bullous pemphigoid without IgG autoantibodies to the BP180 NC16A domain," JAMA Dermatology, vol. 154, pp. 347-350, 2018.Available at: https://doi.org/10.1001/jamadermatol.2017.5465.
[19] A. R. Ahmed, B. S. Kurgis, and R. S. Rogers, "Cicatricial pemphigoid," Journal of the American Academy of Dermatology, vol. 24, pp. 987-1001, 1991.
[20] E. Messmer, C. Hintschich, K. Partscht, G. Messer, and A. Kampik, "Ocular cicatricial pemphigoid. Retrospective analysis of risk factors and complications," The Ophthalmologist: Journal of the German Ophthalmological Society, vol. 97, pp. 113-120, 2000.
[21] J. Brydak-Godowska, J. Moneta-Wielgoś, M. Pauk-Domańska, E. Drobecka-Brydak, A. Samsel, M. Kecik, C. Kowalewski, W. Mackiewicz, and D. Kecik, "Diagnostics and pharmacological treatment of ocular cicatrical pemphigoid," Eye Clinic, vol. 107, pp. 725-727, 2005.
[22] S. B. Khalida, M. Manjunath, A. Annaji, and L. Himanshu, "Benign mucous membrane pemphigoid: Oral, ocular and laryngeal lesions," Journal of Case Reports and Images in Dentistry, vol. 2, pp. 19-22, 2016.